I'm sure you've all heard of photochromic lenses before, the ones that change colour as you move from inside to outside. They may be called reactions, transitions, photochromatic, reactolite or any other name but they're all the same thing essentially. Built into the lens is a substance that reacts to UV light which then causes the lens to darken - the exact mechanism depends on the manufacturer and lens material.
So where am I going with this?
The answer is photochromic clothes. A company called Photochromia have developed a way of inserting photochromic materials into ink used to print onto hats, T-shirts and trousers so now your clothes can change colour when you go outside. Unlike Global Hypercolour (anyone remember that from the 90s) which reacted to heat, therefore showing where and how much you were sweating (ew!) these clothes will react to UV light.
Whilst the designs may not be to everyone's tastes I think some of them are quite funky, especially the idea behind Schrodinger's cat, and it is an interesting use of the technology, it's definitely a whole new take on the term wearable technology. You can read more about it and buy the clothes via their kickstarter page which has reached its target so the clothes will be made. Who knows what designs other companies will come up with and where it will go from here?
Wow, didn't realise it had been that long since I had written an update. It's been a busy 3 months mainly full of revision, revision, more revision and then exams, exams and more exams. However at the end of it all I have finished my 3 years of studying at Cardiff with a 2:1 in optometry and am looking forward to graduating in mid-July.
After finishing all the exams and the obligatory nights out to celebrate, it was time to relax and make the most of the little time I had left with my friends before they scattered to the winds (well South England). So after a quick trip back to Bath and a few rounds of adventure golf it was time to bid everyone fair well, with the stinging words of the sassy Deku tree ringing in my ears.
Why don't you try a game that requires less skill? Like sleeping!
After that, rather than just sit around moping or doing something sensible like relaxing in the sunshine I decided I was going to learn basic level Japanese on an intensive course. I've been interested in Japanese for a while and did a taster session with the Student's Union a few months back and love the culture. Rather than taking the straightforward choice of doing the course in my busy evenings, I took the opportunity to make the most of my last few days of studentship and do the course with the university. It was hard work but good fun so I doubled down and did stage 2 of the beginners course the week after. I'm glad I did it, now just need to keep the knowledge and understanding up and growing.
Right back to the eye related topics from next post.
After handing in my dissertation a week ago - freedom! Last week it was my turn to head off to Bristol Eye hospital to have a look at what happens when we refer a patient and how they are managed under the hospital eye service.
Of course this means having to get up rather early to get to the hospital for 9 am, leaving Cardiff at 7:30 am. I hate early mornings!
The first morning I was in optometry, which for the most part consisted of refraction with a bit of slit lamp funduscopy. Some features of our typical routine seem to go out the window, so no history and symptoms (or fairly minimal), no binocular vision, no motility etc. I suppose a lot of those have been done elsewhere or before so will only be done if needed. In this clinic I got the chance to see some keratoconic patients and see just how the condition affects their vision, recurrent erosion syndrome and an endothelial graft after Fuch's endothelial dystrophy. It was good to see some of these rarer conditions and to see the type of patients that are managed under the hospital.
The afternoon was spent in surgery. After dressing up in some very attractive raspberry scrubs and stylish orange crocs, it was time to go and watch some operations. The first two were fairly simple cataract phacoemulsifications and IOL insertions or in simple terms cataract removal. The last operation was a little bit trickier, the removal of an IOL that had become opacified, so needed to be removed and replaced. This was really interesting to watch to see how the surgeon adapted the procedure. The first two were good to watch to better understand what we would be referred patients with cataracts would undergo, the final operation was just intriguing. You can see what is involved in a cataract operation on the video below (not if you're slightly squeamish).
After another early start on Tuesday, it was a trip to outpatients - in particular medical retina. This clinic featured patients who were being monitored for follow up after treatment at the hospital, but also an inpatient who the doctor had seen earlier in the day. These patients had often been referred from the diabetic screening service (a must for any diabetic patient), but also included branch and central retinal vein occlusions, uveitis and adult vitelliform dystrophy.
The afternoon was spent in a shared care clinic focusing on glaucoma, although neither of the patients we saw in our time there had glaucoma. Instead they had ocular hypertension and were borderline, hence why they were being monitored under the hospital.
The final morning saw a trip to casualty, as an observer not as a patient. This was split into two parts, one watching the optometrist in the eye casualty, the other in the triage station with the nurses. Before we saw any patients I had a chat with the optom and learnt how they got into hospital placement (via independent prescriber is the answer). Then it got interesting - a patient with a large patch of their corneal epithelium missing after being poked in the eye by their 14 month old son, suspected uveitis and then a retinal detachment complete with tobacco dust. With the nurses I got to see how they triage patients; check vision, quick slit lamp exam and what they are able to do - remove small foreign bodies, give out drugs, refer to different departments as necessary. Patient wise I saw some interesting cases, 5 corneal ulcers on same eye (!), a foreign body due to a granule from an exfoliating facewash and chemosis (which looks worse than it is).
Overall I really enjoyed my time at the hospital (despite the early starts) and it's made me think a little more about what I want to do after I qualify. I would like to thank all the staff at the hospital for putting up with all us students asking stupid questions and getting in the way and the patients for letting us have a look at their eyes despite some serious conditions.
This is a slight departure from my normal, irregular ramblings in that it isn't directly about optometry, rather it's about something I got up to this last week and feel strongly about.
Reclaim the night is a series of marches in various cities to highlight the issue of violence against women and how they don't feel safe walking the streets at night (and at times during the day). The movement started in the 1970's in response to police telling women to stay off the streets as the Yorkshire ripper was still at large. Since those days the rape conviction rate has remained extremely low, with only 1070 convictions in 2013/2014 despite 12,000 men and 85,000 women being raped.
While I may not be able to stop people being raped in person, I can help highlight the issue and do my best to help cut down the prevailing "lad" culture. This makes some men foolishly think that it is okay to grope, harass, cat-call and intimidate women all in the name of "banter". This is no better exemplified by Dapper Laughs who was due to perform at Cardiff University Students Union on Friday before a successful campaign to stop him performing at the Union by one of the guest speakers (you can read more about that here and here).
Women shouldn't have to be afraid to walk the streets at night for fear of attack. They shouldn't have to put up with being groped in night clubs, they shouldn't be afraid to say no to men and they shouldn't be blamed if a man attacks them. Alcohol, what they are wearing, where they are - nothing is an excuse for a man to attack a woman EVER!
Because of this I took part in the Reclaim the Night Wales march held in Cardiff last Friday. The event was organised by NUS Wales and included students from Cardiff University, other universities and the rest of Wales. After making banners we walked round Cardiff city centre making a lot of noise and drawing a lot of attention to highlight the issue as much as possible. This was followed some very brave and thought provoking speeches back at Y Plas.
I am proud to identify as a feminist and commit to doing my best to raise awareness of the issues that women face and trying to stamp out sexist behaviours whenever I encounter them.
It's now three weeks into 3rd year and I've just about survived all my clinics without killing, hurting or mentally scarring my patients (I think I have anyway).
I'll start with the lectures, they've been challenging, interesting and scary at the same time. From the sheer amount of detail in abnormal ocular conditions to the real life knowledge of occupational optometry via the life changing low vision and special assessment. First year is all about bringing everyone up to the same level and getting people used to the university way of teaching whilst instilling basic principles and some background knowledge. Second year builds on this and you start to learn practical applications such as binocular vision and contact lenses. Third year is where it all comes together, it's all about applying principles in practice and smoothing out the rough edges in knowledge and patient interaction. It is knowledge gained in third year is what I will be using on a daily basis in my future career, assuming it actually goes into my brain.
Onto clinics, which are the main part of the third year, I've had 2 primary care patients, 1 contact lens patient, sat in on 3 special assessment clinics, done 2 dispenses and 1 collection. What have I learnt from all that? That at the moment I am nowhere near ready to see patients unsupervised or finish my degree. Have they really been that bad, probably not but they have certainly shown how much more I have to learn. The main problem has been me getting myself into a flap and not following a logical order with tests or allowing small little things to throw me and knocking my confidence for the rest of the test. Both my first contact lens and primary care were a bit of a fluster and whilst I recovered in primary care, I was still a mess at the end of my contact lens clinic. Thankfully I had a really nice patient who knew what they were doing for the teach but it still really annoyed me that I was such a mess. The plan, is to create a little crib sheet so that I have something to refer to if I lose the plot again. I don't intend to constantly refer to it, that would ruin the flow of the test but at least it gives me a fallback and hopefully writing it out will settle things in my mind better. The other main learning I have taken away from primary care is the need to refine my funduscopy technique with Volk style lenses, I should have plenty of time for that during my dissertation (more on that in a bit).
Special assessment has been the most challenging clinic but the most rewarding at the same time. I've seen three very different patients, a young child with Down's, a 44 year old with severe learning difficulties and a 14 year old who really didn't need to be in the special assessment clinic. The tests have shown just how much a simple eye test can vary based on the patient, from using glowing gloves as a fixation target for ophthalmoscopy to having music on to calm a patient down so you can test them.
Finally my dissertation: "Can an everyday mobile phone camera be used to image
the retina instead of an expensive commercial retinal camera?". This was my first choice based on my previous history with mobile phones and I'm really looking forward to the challenge and gaining the experience with Volk style lenses. I've got lots of ideas where to take this, possibly too many for the time and word count I have for the project but it's going to be fun.
So after a busy summer of working various placements I do have an offer for a pre-reg position, a new weekend job and a slightly healthier bank balance even if I would have preferred to have a little more time to relax. Now however it is almost time for third year to begin.
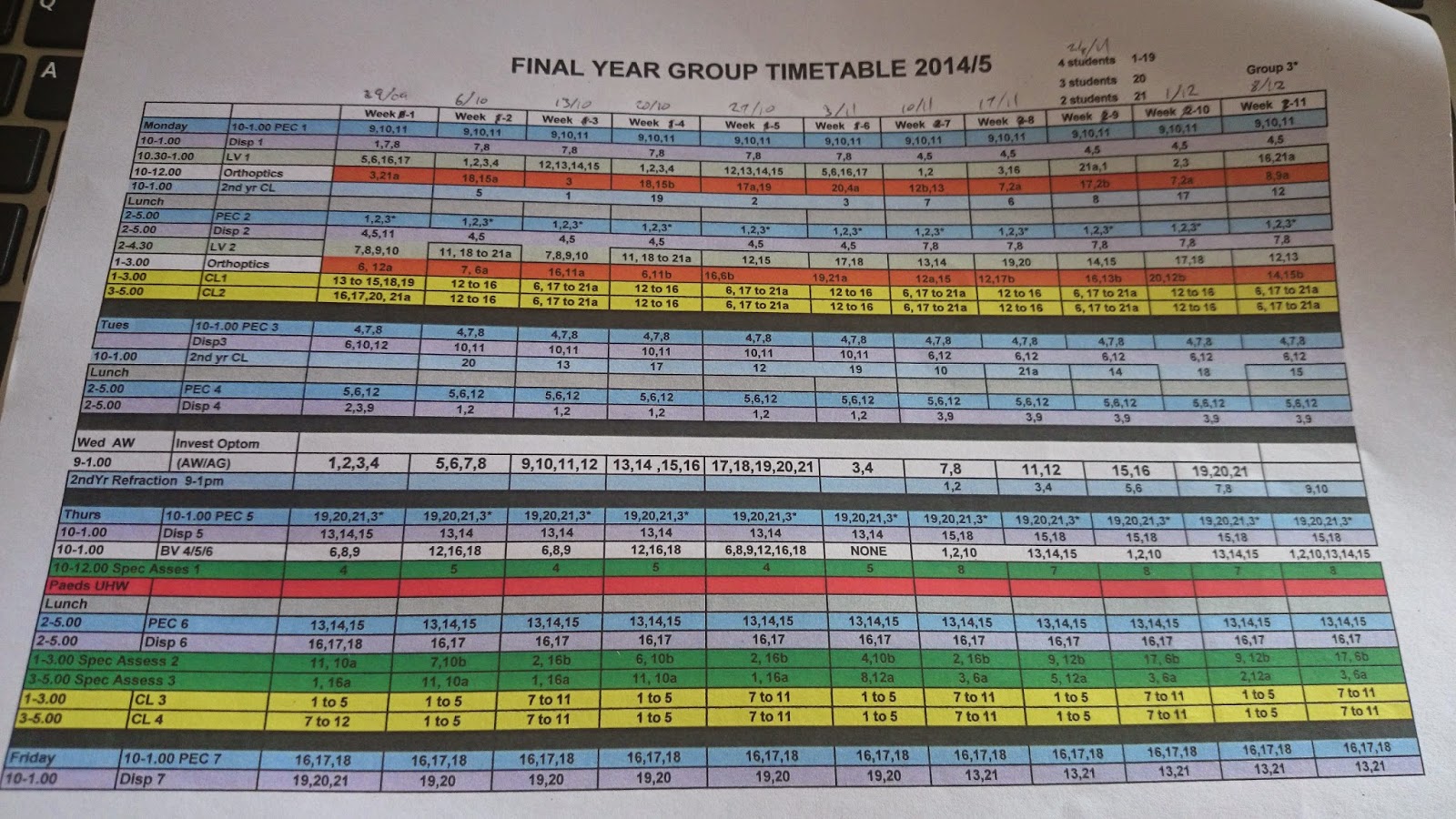
Last week was Freshers week, my 7th in total, and I managed to survive (just) despite having a cold develop and being knackered the entire week. Wednesday especially I was walking round like a zombie for no real reason. The week was spent organising OPSOC and signing up members, new merchandise launches on Monday and then getting and trying to decipher my clinic timetable.
Seriously?!
To be fair it's not that bad once you figure out the pattern and know which group you're in but just a bit scary the first time you see it. Overall mine isn't too bad apart from a few Thursdays towards the end of term when I go 9-6 straight with no breaks - it's going to hurt!
I am looking forward to starting back again, seeing real patients and learning more, although the first few weeks maybe a bit sketchy. The main thing I want to know is what I am going to write my dissertation on, get that in a week or two, as I actually want to start writing it mainly as I have a feeling the second semester is going to get hectic. I will probably not be saying this once I have the title and started it but that's life.
Today I have been helping out as a victim, sorry volunteer, for a summer research project at Cardiff university. These projects are undertaken by students between second and third year to help gain an insight into research ready for third year projects and to see if a PhD or Masters would be something they would be interested in. The projects also help to keep Cardiff at the leading edge of eye based research that the school of Optometry and Vision Science is so renowned for.
Today I have been helping with a project funded by Coopervision being conducted by one of my friends comparing the effects of over the counter blepharitis treatment compared to baby shampoo. In particular it is looking at the effects of the scrubs on ocular comfort and staining. This has resulted in me having fluoroscein and lissamine green put into my eyes, leading to me having a fetching shade of green eyeshadow for most of the day.
Still it's a small price to pay to help for driving research forward.